IZERVAY My WaySM is a patient support program customized to your unique patient-access needs.
Benefits
Investigations
Affordability
Options*
Prior Authorization
Support†
Patient Assistance
Program*
Appeals/Denials
Support†
Product
Replacement*
*Subject to eligibility requirements. Void where prohibited by law. See complete terms and conditions available at IZERVAYecp.com/PatientSupport, or reach out to your Access Coordinator.
†The healthcare provider remains responsible for populating all clinical documentation.
Initiation
76%1‡
of surveyed customers found initiation for IZERVAY easy
Speed
0.5 days1§
average benefit investigation turnaround time
Programs
80%1‡
were highly satisfied with IZERVAY My Way patient support services
‡Based on Awareness, Trial, and Usage (ATU) survey of 50 customers, October 2024.
§Based on benefits investigations conducted by IZERVAY My Way, February 2025.
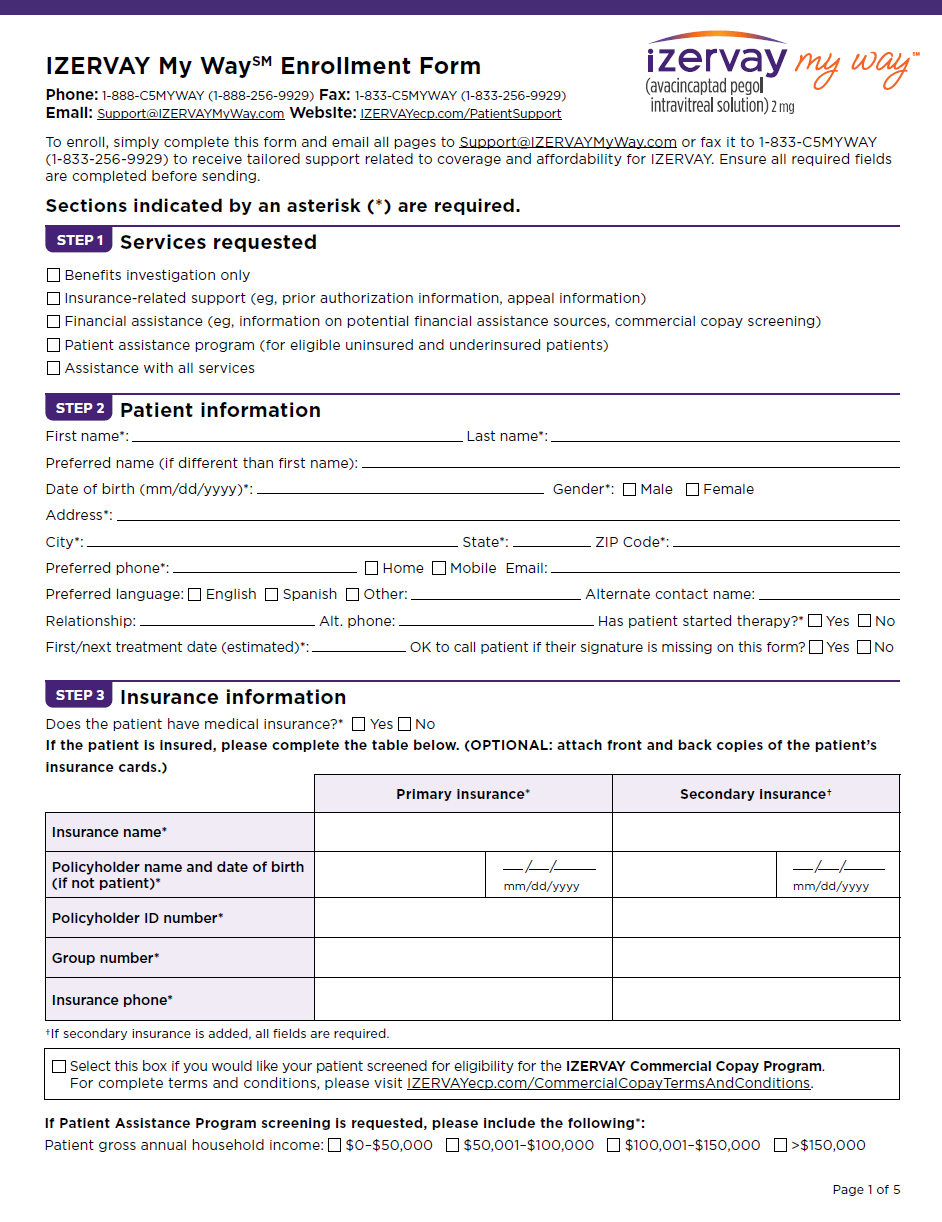
Get started today. Complete IZERVAY My WaySM enrollment in any of the following ways:
The IZERVAY My WaySM portal is your place for all access and affordability solutions for your patients prescribed IZERVAYTM.
OR
Download the enrollment form and submit it via email or fax
If you need assistance, please don’t hesitate to contact our team for live support. Phone: 1-888-C5MYWAY (1-888-256-9929) 8 AM to 8 PM ET Monday – Friday
Once your patient is enrolled, a dedicated Access Coordinator will reach out to you to help your patient get started.
Our broad distribution network is designed to accelerate access.
Fax: 614-553-6301
Fax: 800-862-6208
Fax: 888-752-7626
Fax: 800-800-5673
IZERVAY is also available through a broad open network of specialty pharmacies if mandated by a patient’s health plan. Be sure to contact the specialty pharmacy to confirm availability.
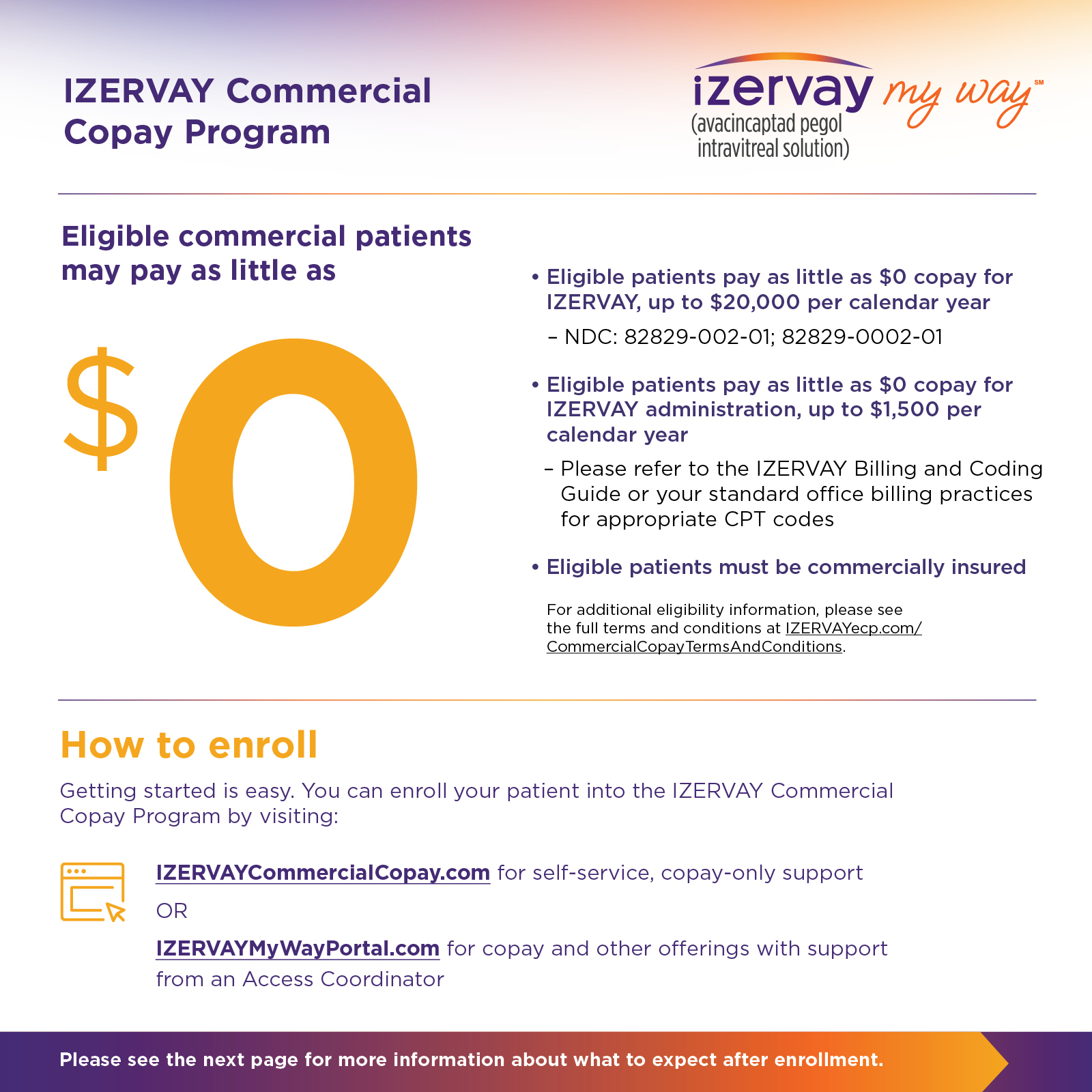
Discover affordability options for your patients across insurance types.
Visit IZERVAYCommercialCopay.com for self-service, copay-only support.
Enroll your patient into our IZERVAY My WaySM program for copay and other offerings with support from an Access Coordinator.
Patient assistance program
Financially eligible patients may be able to receive IZERVAY at no cost.
Click here to view terms and conditions.Enroll your patient into our IZERVAY My WaySM program for copay and other offerings with support from an Access Coordinator.
Download the Billing and Coding Guide for helpful information on coding and billing for IZERVAY
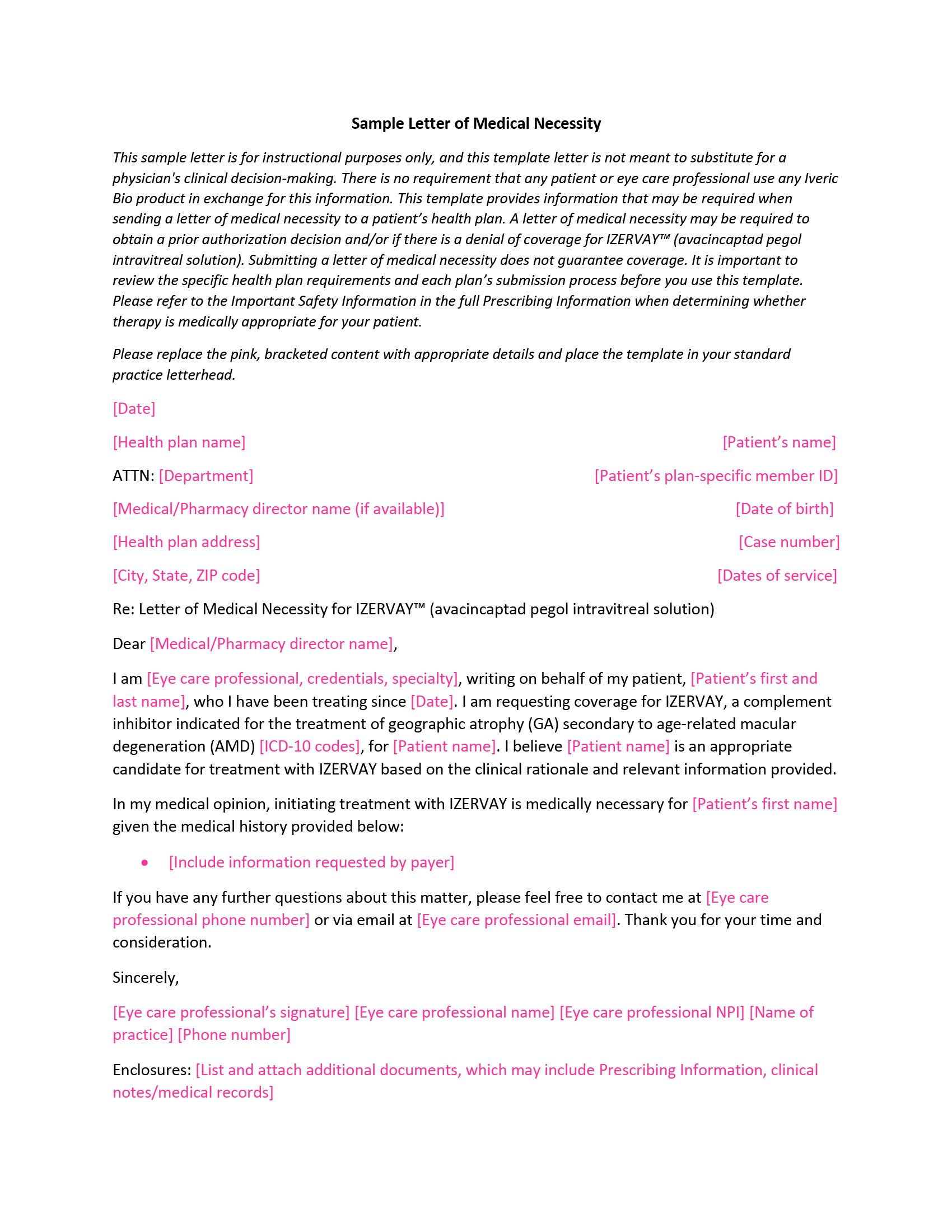
Downloadable Resources
Resources are available for you and your patients throughout their treatment experience.